The short answer is no.
Pain is not a measure of bodily damage. Rather pain is a response that the brain creates to motivate you to protect yourself when the stimuli it receives are interpreted as dangerous. Pain is an output, not an input [1,2].
Sensation vs Perception
Heat, cold, pressure, sweetness, light, vibration etc are senses*. That is to say, we have a specific sensor for these inputs in the environment. The brain takes this sensory information and creates a perception. It is this perception that we are aware of, not the actual sense itself. Some perceptions have distinct motivational qualities, and these I will refer to as Urges.
Pain is just such an Urge, it is a motivator, an appetite. Hunger urges you to eat, pain urges you to protect the painful area. Urges like hunger, thirst, libido and pain are the result of the brains evaluation of multiple inputs.
Of course, hunger itself is not a reliable measure of actual calories needed, many things besides a need for calories can stimulated hunger. This is demonstrated by studies showing how kids eat 45% more snack food when watching a tv show that has food commercials [3], that overweight people are more likely to eat more when there is more food on the table, and that time of day , sweetness, packaging and variety can all stimulate hunger [4]. Your brain evaluates all the available information to determine whether or not to create the urge to eat, ie hunger. Some of this information comes from your own body (fullness of stomach, insulin levels etc) and some comes from your environment (availability of food, signals of future food insecurity, smells etc). And yet even if you know that your hunger was triggered by an external stimulus like an advertisement, you still feel hunger and really want to eat.
Like hunger, pain is the result of the brains evaluation of many inputs, of which bodily injury is only one. Even if you know it is caused entirely by inputs that are independent of bodily damage, you still feel pain and really want to protect yourself.

Although our eyes sense light/dark and color, what we “see” is ultimately a created by our brain, it is a perception as the following illusion illustrates: The two blocks appear to be different shades, but place your finger horizontally across the line between the two blocks and you will see that they are actually the same color [28].
What Causes Pain?
The brain adds up all the danger signals and the safety signals and when the former outweighs the latter it creates pain [1]. The brain ads up both the internal (bodily) inputs and the external (environmental) [1]. If you are feeling pain, it is because at this moment your brain has determined there are more danger signals than safety signals and protection is the priority. This model of pain is called the “protectometer” by Lorimer Moseley [1].
Is Pain Really Not a Reliable Measure of Bodily Damage?
There is an overwhelming amount of evidence documenting the disconnect between damage and pain. This evidence is summarized as follow:
Bodily Damage without Pain
- Patrick Wall and Bill Noordenbos examined 73 Israeli soldiers with traumatic amputations in the Yom Kippur war. All of them reported surprise that the felt no pain at the moment of injury. A prior study by Harry K. Beecher at the Anzio Beachead in WWII found that 70% of the injured soldiers did not feel pain. This lack of pain was not due to shock or disorientation as the amputees were cognitively intact.
- About 1 in a million people are born without the ability to create pain from physical stimuli [5]. Having two defective copies of the SCN9a genes is one way this can happen [6]. Other’s with congenital insensitivity to pain have PRDM12 mutations.
- Phineas Gage had a railroad spike blown through his brain, destroying his left frontal pain [7]. He is reported to have felt no pain. Recently a similar injury happened to Brazilian construction worker Eduardo Leite who also reportedly felt little pain despite his massive injury [7].

Illustration of Phineas Gage’s injury [32].
Pain without Bodily Damage
- Bend your first finger back, bend it further, keep bending it until it hurts, then let go. Chances are, your finger was not damaged in this process. Most people’s brains create pain in response to the intense stretch well before any tissue injury occurs. People differ, and some brains will cause pain far in advance, whereas others will not create pain until the very brink of damage or beyond [1].
- Numerous pain studies use carefully controlled electric shocks to induce pain without causing damage.
- In the Yom Kippur War study mentioned above, 65% of amputees experienced phantom limb pain 24 hours after the injury. They felt pain in the hand or foot that was no longer there.

[33]
Pain can be reduced by a long list of interventions that have no direct effect on the injured area
- Opiate medications are the most effective and widely used analgesic yet they are not currently known to play a direct role in the healing process [8].
- A placebo pill provides as much headache pain relief as aspirin but not as much as ibuprofen [9].
- Branded aspirin provides better headache pain relief than the same medication with a generic label, especially for those who regularly use that brand [10]. A placebo described as being the active medication worked just as well at reducing headache pain as the active medication being described as a placebo [12].
- Branded placebos provided equal headache relief as generic labeled ibuprofen and better pain relief than a generic labeled placebo [11].
- Fake arthroscopic surgery was equally effective as the real thing for knee osteoarthritis [13].
- Injections of placebo provided slightly better headache relief (32.1%) than placebo pills (25.7%) [14].
- Colorful capsules provided better pain relief than a monochromatic ones [15].
- Sham acupunture provided more pain relief than a placebo pill [16].
- Acupuncture needles placed in random points is equally effective at reducing pain as needles inserted at traditional Chinese medicine points [17]. Other studies have shown true acupuncture to be slightly better than sham (1 point more pain relief on a 1-10 scale) [18].
- Face to face pain neuroscience education has a small independent pain reduction effect on patients with fibromyalgia [19] but a booklet with similar information had no effect [20].
- Sham brain stimulation relieves pain [23].
Pain can be increased by a long list of interventions that have no direct effect on the injured area
- People with chronic neck pain reported pain while turning their neck in virtual reality according to what appears to be the same amount of neck rotation that usually hurts. If their neck typically hurt at 45 degrees of rotation and the virtual reality glasses make it look like they were at 45 degrees when they were actually at 35 degrees, they reported pain at 35; if the glasses make it look like they were at 45 when they were actually at 55, they didn’t report pain until 55 degrees [21].
- The same 20deg celsius cold metal wand on the back of the hand hurts more when there is a red light on the wand than when there is a blue light. Furthermore, it feels hot when there is a red light, even though it is cold [22].
- When people are placed in a “brain stimulator” and asked how much pain they feel, their pain is proportional to the stimulator’s intensity dial placed in front of them. Atlhough the stimulator looks real, it is actually a sham, is not plugged in and the dial is not connected to anything [24].
- When patients with complex regional pain syndrome had their painful hand placed in a mirror box and then watched the reflection of their non-painful hand being touched in the place where their painful hand would hurt, they felt pain in their painful hand. Pain in the painful hand was elicited by touching the other hand [25].
- The flexion withdrawal reflex from a noxious stimulus such as an electric shock on the foot is greater when a bad odor is placed under the nose [26].
- In “the rubber hand illusion” once someone believes the rubber hand is their own, their body reduces blood flow to their real hand and it becomes cold. When you appear to injure the rubber hand, they feel pain [27]
- When the side effects of a medication are described as being potentially severe due to the drug being powerful, more pain relief is achieved. But even placebo’s can cause the side effects that they are described to have. [9,29]
- The feeling of stiffness in the back doesn’t correlate well to actual mechanical stiffness. This feeling of stiffness is greater after people hear the sound of a creaky door. [I heard this in Lorimer Moseley’s talk at CPTA 2015 but couldn’t find the original source].
- The hand withdrawal reflex amplitude is greater after people have been shown a picture of a hand being mutilated in a meat grinder but the leg flexion withdrawal reflex is unchanged after this picture. [I heard this in Lorimer Moseley’s talk at CPTA 2015 but couldn’t find the original source].
- On day two after an ankle sprain there is hypersensitivity (allodynia) in uninjured parts of the ankle. [I heard this in Lorimer Moseley’s talk at CPTA 2015 but couldn’t find the original source].
- On day four after an ankle sprain there is hypersensitivity (allodynia) on the other ankle at the same location as the injured side. [I heard this in Lorimer Moseley’s talk at CPTA 2015 but couldn’t find the original source].
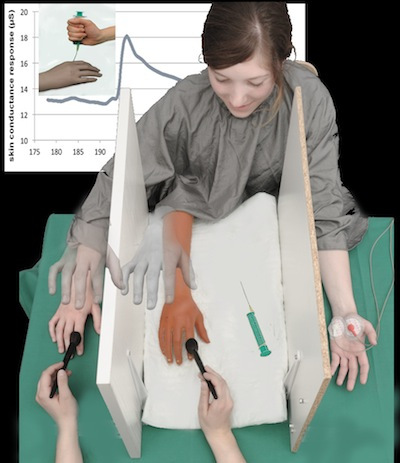
Illustration of the rubber hand illusion [34].
What about “listening to your body”
The challenge with “listening to your body” in the current environment is that these basic motivations such as hunger and pain can be distorted and lead us to behaviors that are not in our long term best interest. Many overweight people really do feel hungry all the time despite the clear evidence that they are eating more than they need and by listening to their body they continue to gain weight and worsen their health. Many people in chronic pain, really do feel pain all the time but without any biologically significant damage that needs protection. As a result they restrict their activity and worsen their health [30]. This self destructive behavior can be completely unintentional. They are only following the powerful motivation systems they were hard-wired with.
So When Does Pain Mean Damage?
In the middle of a marathon it would be nice to know if that burning pain above your heel is just strain amplified by your memory of your dad’s achilles tear or the tissue damage of your own impending tendon rupture. This is not a hypothetical question, I have seen people run through pain and rupture tendons, and three years, six surgeries and a lot of pain later they are unlikely to ever run the same again.
Below are my current thoughts on how to infer when such damage is present and thus modify one’s activity. This is an evolving framework and I welcome your comments.

It would be nice to know before your tendon looks like this. Unfortunately, achilles tendon ruptures often occur suddenly with no prior warning [37].
#1 Look for these other signs of damage:
- Visual signs: bleeding, open wound, bruising, significant swelling, disfigurement, hearing bones crack or tendons snap
- Functional signs: inability to move a body part, prolonged loss of sensation*, loss of range of motion
- Imaging: Ultrasound, CT, x-ray and MRI can all show signs of damage. MRI is the most accurate means of determining if inflammation is present. Local inflammation usual occurs after tissue damage, although recent research has revealed how stress and diet can increase the inflammatory response.
I feel that it is no coincidence that the most common chronic pain conditions in the world lack most of these reliable signals of damage: headaches, fibromyalgia, headaches, neck and back pain. The most common areas of chronic pain are usually deep and can’t be directly seen without a mirror. I think that without any confirmation of the extent of damage or recovery of damage (seeing a wound heal for example) the anxious mind can imagine the worst. The exception to this of course is post-surgical complex regional pain syndrome.

[35]
#2 Look for these injury histories that suggest damage:
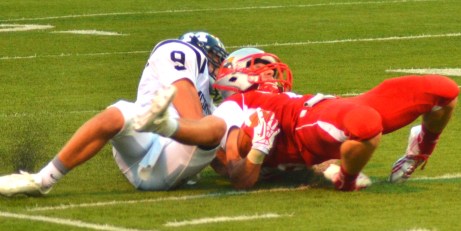
- There was a clear moment of high-impact mechanism of injury (car accident, fall, a large dog barreling into your knee)
- The pain occurred simultaneously with or immediately after the suspected mechanism of injury and then worsened over the next 24-72 hours. This worsening is due to sensitization of the nerve endings by bradykinin as part of the inflammatory response.
Here things start to get tricky. A common situation is one in which someone goes through their day without any pain, then the next day they wake up with pain. Did they sleep in an awkward position or did they injure themselves the day before? We will never know for sure, but there are clues. If you repeat the suspected movement and it worsens or increases your pain, then it is more likely that that movement caused some bodily damage. A sharp or sudden pain, with no pain afterwards is less likely to indicate damage than pain that began the day after the suspected cause and can be worsened by repeating the movement or posture.
[36]
#3 Adjust your caution by the pain location.
Not all damage requires protection, only damage that if left unchecked would result in worse long-term bodily function. Some areas of the body have poor healing capacity and thus it is prudent to have a more cautious approach to pain in these areas. I have ordered the following locations from least regenerative, and thus warranting the greatest caution, to most regenerative where pain warrants the least caution.
- Non repairing
- Meniscus & Labrum
- Scarring but not regenerating
- Inter-vertebral Discs
- Articular Cartilage
- Complete ligament and tendon tears
- Partially regenerating
- Partial ligament and tendon tears (depends)
- Brain and Spinal Cord
- Nerve severing (neurotmesis)
- Fully regenerating (small injuries heal “good as new,” scar tissue may remain for larger injuries)
- Nerve Crush (axonotmesis)
- Bone (with the exception of some non-healing lesions)
- Muscle & Fascia
- Skin
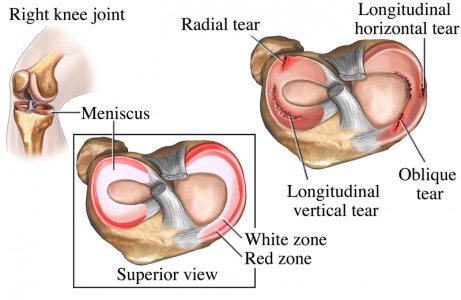
Most meniscus injuries do not repair themselves. That being said, many people go on to be symptom free after a meniscus tear [38].
Look for other danger signals that may be amplifying your pain
Refer to the list above in “Is pain really not a reliable measure of bodily damage” to see all the stimuli that have been shown in research to increase pain without worsening the injury (and increase pain even when no injury is present). Many of the things that have been found to cause or worsen pain involve signals of danger or believes about injury. The stimuli that contribute to pain may be unique to you. The Protectometer workbook is one way to help identify what is triggering your pain.
[1]
What should we do about pain?
First, if you are in pain, find a trusted healthcare provider to help you figure out what is going on. If your pain changes with movement or bodily position, see a physical therapist.
It would be nice if we had some sort of separate “damage-o-meter” that could tell us when tissue damage is present and help us make decisions about activity modification. In the future perhaps such a device will be available. For the time being we are left with pain as a messy and unreliable measure of damage. I hope that this article has brought your understanding of pain closer to the current understanding of modern neuroscience research and that your life will be enriched because of it.
Appendix
* The list of sensor types that have been discovered in the human body is remarkably long.
References
- Explain pain : The Protectometer (2015) by David S. Butler, G. Lorimer Moseley
- Explain pain. (2013) by David S. Butler, Moseley
- Harris JL, Bargh JA, Brownell KD. Priming Effects of Television Food Advertising on Eating Behavior. Health psychology : official journal of the Division of Health Psychology, American Psychological Association. 2009;28(4):404-413. doi:10.1037/a0014399.
- Wansink B. Environmental factors that increase the food intake adn consumption volume of unknowning consumers. 2004.
- The Independent. The people who can’t feel pain: Scientists discover cause of rare inherited condition that turns off pain sensors. 2015
- Cox JJ. An SCN9A channelopathy causes congenital inability to experience pain. Nature. 2006
- Eli MacKinnon. Modern Day Phineas Gage? How a man survived a rod through his brain. livescience.com 2012
- Ream Al-Hasani Molecular Mechanisms of Opioid Receptor-Dependent Signaling and Behavior. 2013
- Diamond S. Ibuprofen Versus Aspirin and Placebo in the Treatment of Muscle Contraction Headache 1983
- Branthwaite Analgesic Effects of Branding in Treatment of Headaches. 1981
- Faasse Impact of Brand or Generic Labeling on Medication Effectiveness and Side Effects 2015.
- Kam-Hansen Altered Placebo and Drug Labeling Changes the Outcome of Episodic Migraine Attacks. 2014
- Moseley. A Controlled Trial of Arthroscopic Surgery for Osteoarthritis of the Knee. 2012
- Craen. Placebo effect in the acute treatment of migraine: subcutaneous placebos are better than oral placebos. 2000
- de Craen AJ, Roos PJ, Leonard de Vries A, Kleijnen J; Roos; Leonard De Vries; Kleijnen (1996). “Effect of colour of drugs: systematic review of perceived effect of drugs and of their effectiveness”. BMJ 313 (7072): 1624–6.
- Kaptchuk T, Stason W, Davis R, Legedza A, Schnyer R, Kerr C, Goldman R. Sham device v inert pill: randomised controlled trial of two placebo treatments. BMJ (Clinical Research Ed.)2006;332:391–397. [PMC free article] [PubMed]
- Colquhoun. Acupunture is a Theatrical Placebo. 2013
- Moffet. Sham acupuncture may be as efficacious as true acupuncture: a systematic review of clinical trials. 2009
- Oosterwijck. Pain physiology education improves health status and endogenous pain inhibition in fibromyalgia: a double-blind randomized controlled trial. 2013
- Ittersum. Written pain neuroscience education in fibromyalgia: a multicenter randomized controlled trial. 2014
- Harvie. Bogus visual feedback alters movement-evoked pain onset in people with neck pain. 2014
- Moseley. The context of a noxious stimulus affects the pain it evokes. 2007
- Marchand. Analgesic and placebo effects of thalamic stimulation. 2003
- Bayer. The role of prior pain experience and expectancy in psychologically and physically induced pain. 1998
- Acerra. Dysynchiria: watching the mirror image of the unaffected limb elicits pain on the affected side. 2005
- Bartolo. Modulation of the human nociceptive flexion reflex by pleasant and unpleasant odors. 2013
- Capelari. Feeling pain in the rubber hand: integration of visual, proprioceptive, and painful stimuli. 2009
-
Rosenzweig. The placebo effect in healthy volunteers: influence of experimental conditions on the adverse events profile during phase I studies. 1993
-
Fine PG. Long-term consequences of chronic pain: mounting evidence for pain as a neurological disease and parallels with other chronic disease states. 2011.
-
Phineas Gage by Jedimentat44. Creative Commons Attribution License 2.0
-
My Nasty Ankle. Shane Adams. Flickr Creative Commons Attribution License 2.0
-
Mentor Cardinals vs Erie McDowell Trojans by Erik Drost. Flickr Creative Commons Attribution License 2.0

{kind=link}
{kind=link}
{kind=link}
Pingback: Reducing Pain by Managing Stress with Technology | Posture Movement Pain
Pingback: If I have too much curve in my back will it cause back pain? | Posture Movement Pain